Mental Disorder: A Perverse Social View

The work of psychologists has been attacked on many occasions and from numerous fronts – to our sadness, not always unfairly. It suffered from popular myths, internal debates, different currents, ignorance or the daring of those who announced wisdom without knowledge. Not to mention professional opportunism, the reproduction of models or the great laziness of establishing strong methodological bases before starting an investigation. This problem had no trivial consequences: it directly affected the social concept of mental disorder and all people who live with some kind of disorder.
Furthermore, in psychology there is the false paradox of learning by involvement. It would not occur to any friend to operate on an appendicitis without having studied medicine, no matter how much one day he had suffered from this disease. However, there are many people who write about depression, validating their speech or their cookbook about the suffering they once managed to leave behind. They even believe that a model, which is logical for them, established from personal experiences, is perfectly applicable to everyone. What you have to do is… (and add what they want).
It’s a temptation to complete the sentence…

A different view of psychology
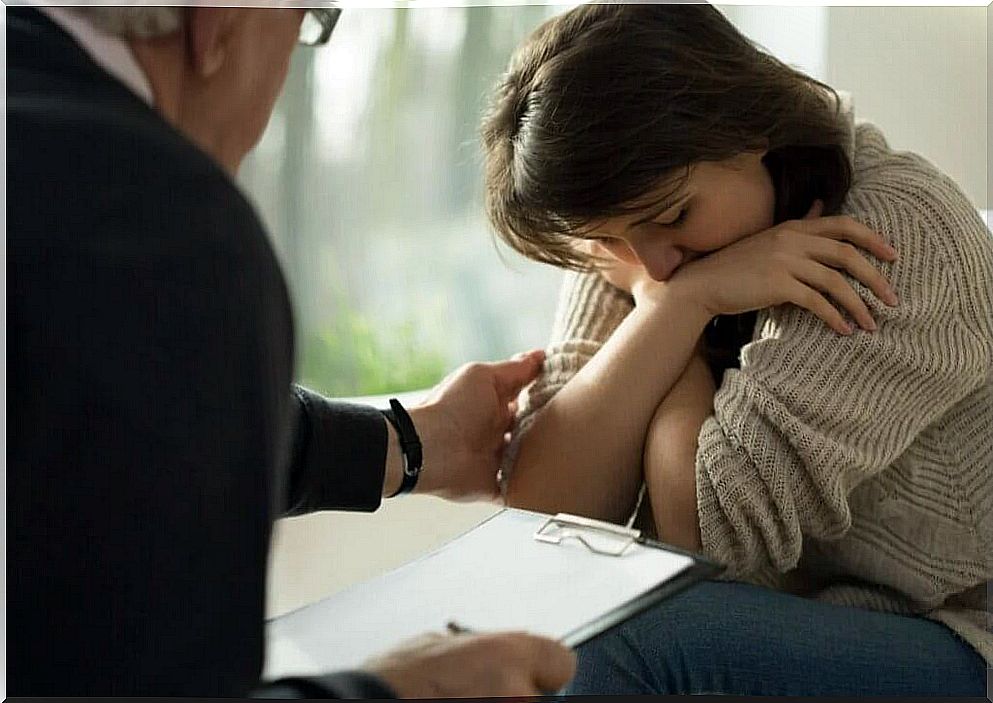
Until recently, those who sought the advice of a friend were considered normal and those who knocked on the psychologist’s door were the crazy ones. Consultations, diagnoses and interventions were camouflaged as the dust was hidden under the rug when visitors arrived. The fear associated with confession was that of rejection, of becoming the center of neighborhood gossip – or, in the modern world, on social media or message boards.
Fortunately, this is changing and the professional psychologist seems to be getting closer and closer to “normal life”. Mental health is no longer just a guarantee of professional success – that story of emotional intelligence or the ability to defer rewards as indicators of success. Today, it goes even further, as it is a source of well-being. Being and feeling good is an investment, just as we do in our body, on a more physical level, playing sports or taking care of food.
The people who lived through this period of darkness for psychology, the main ones affected, were the ones with a mental disorder. Let’s take an example to understand it better. It’s not original, I took it from a dialogue in Lousie Penny’s novel titled Still Life – highly recommended for any reader who loves mystery novels.
The first paragraph looks like this:
– A few years ago, I was a psychologist in Montreal. Most people knocked on my door because they had been through a crisis, and most of those crises boiled down to losses: loss of a marriage or an important relationship, loss of security, job, home, parent, or a mother. Something made them ask for help and look inside themselves. And often the trigger was change or loss.
– And are they the same thing?
– They can be the same thing for someone who doesn’t have the facility to adapt.
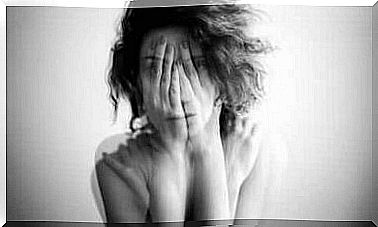
I collected this testimony from this literary psychologist because it largely reflects superficial social perception. I say superficial because the common denominator, the impulse to ask for help, is not born out of loss , but out of suffering.
A suffering that, on the one hand, is not exclusive to those who cannot easily adapt. On the other hand, the use of a resource, such as the consultation with a psychologist, is a sign of adaptation in most cases.
The patient is to blame for his mental disorder
The dialogue continues and reaches the most interesting and dangerous point. The psychologist/librarian in the novel says: “After spending twenty-five years listening to his complaints, I finally closed my doors. I woke up one morning and saw something that didn’t sit well with a forty-five-year-old client who acted like he was sixteen.
Every week he came with the same laments: “Someone hurt me, life isn’t fair, it’s not my fault.” I spent three years proposing things to him, and during all that time he didn’t do anything. So that day, as I listened to him, I suddenly understood: it didn’t change because I didn’t want to, I had no intention of doing it. We were going to keep playing the same farce for another twenty years. And, in that instant, I realized that most of my clients were exactly the same”.
Along these lines, she makes a mistake when referring to a myth: the premise that those who do not find relief -cure- for a mental disorder do not do so because of the absence of desire or will. Because the secondary gains of the person’s situation are powerful enough to make any attempt at intervention fail. In other words, the suffering does not reach the point of making the patient/client/person consider – invest efforts in… – adopt changes that make their customs/habits/dynamics more adaptive.
We are talking about a very dangerous conceptualization of mental disorder. Whether by omission or commission, this way of looking at reality ends up putting the patient/client/person at fault for their non-recovery. Thus, when being guilty/responsible, he would not be worthy of the attention he could receive from the environment or from the resources that the system could make available to him.
“Whenever he wants… he will change”, many people think. Perhaps this is one of the most perverse phrases.